






Medical device enclosure projects often face a difficult balance. The product needs to look professional, assemble reliably, protect internal electronics, and support regulatory or clinical validation schedules. At the same time, the project team may still be validating demand, adjusting the design, or preparing for a future production mold.
In this stage, a full dedicated injection mold may not always be the most practical first step. For suitable enclosure designs, shared mold base tooling can provide a faster and more economical path from engineering prototype to molded parts.
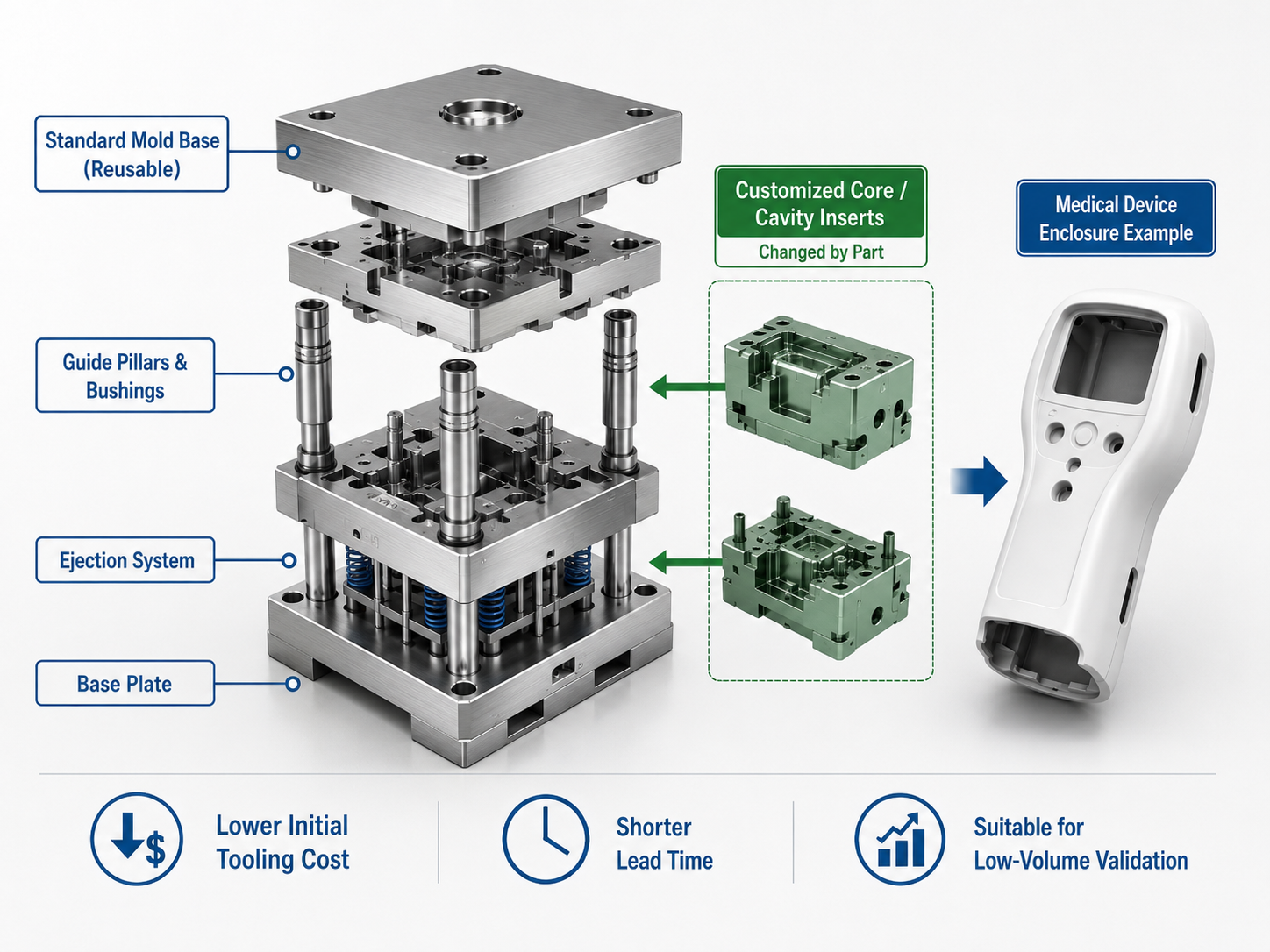
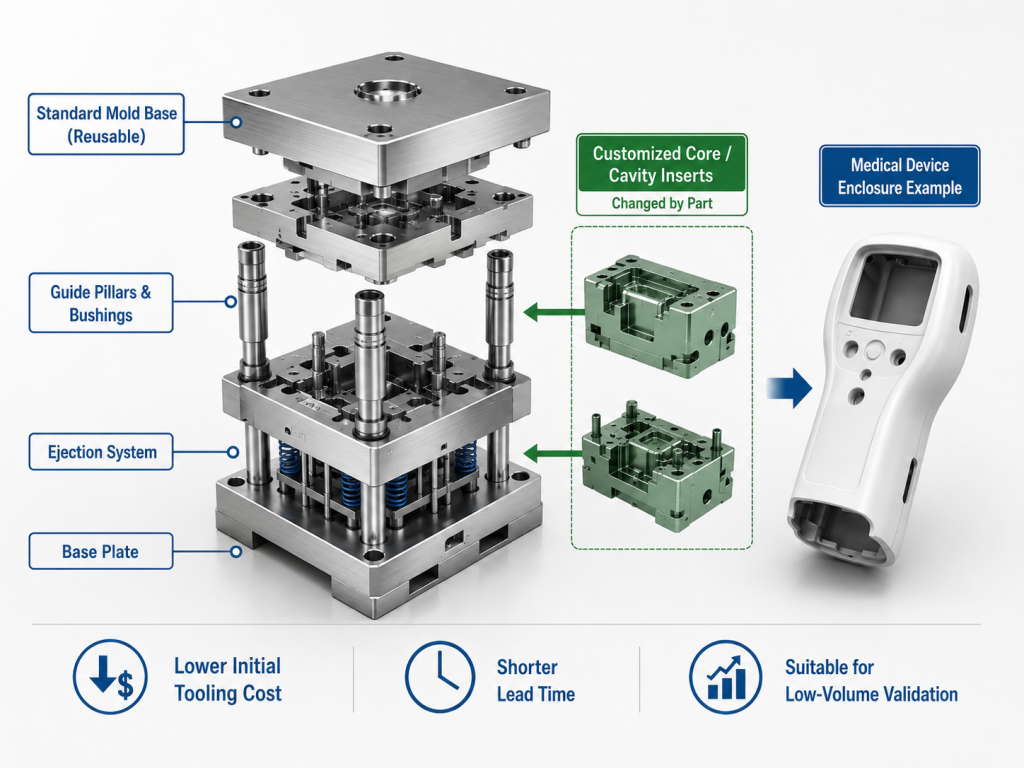
This approach does not mean using a “simple mold” or lowering engineering standards. It means reusing a standardized mold base while customizing the core and cavity inserts that directly form the plastic part. The key benefit is that the project avoids unnecessary mold base investment during early validation. In many suitable cases, this can reduce initial tooling cost by approximately 30%–50%, while still producing injection molded parts for functional, assembly, and market testing.
However, shared mold base tooling is not suitable for every medical enclosure. It must be evaluated case by case, considering part size, structure, cosmetic requirements, undercuts, material, quantity, and expected tooling life.

What Shared Mold Base Tooling Means
In a conventional dedicated mold, both the mold base and the forming inserts are designed for one specific product. This gives maximum flexibility, but it also increases cost and lead time.
In a shared mold base solution, the standard mold base is reused. Components such as clamp plates, guide pillars, guide bushings, and standard support structures are already available. The customized work is concentrated on the core and cavity inserts, cooling layout, gating concept, ejector design, and part-specific machining.
For medical device enclosure projects, this approach is most useful when the design is already close to injection molding requirements but does not yet justify a full production mold. Typical use cases include:
- Engineering validation builds
- Clinical evaluation samples
- Pilot production
- Low-volume market launch
- Bridge production before a dedicated production mold
The value is not only cost reduction. It also helps the customer test real molded parts earlier. Compared with CNC prototypes or 3D printed parts, injection molded samples can better reflect shrinkage, warpage, weld lines, texture, snap-fit behavior, insert assembly, and production-level material performance.
The Best Application Zone
Shared mold base tooling works best in a defined engineering window. A good candidate is usually a small or medium-sized enclosure component, with controlled geometry, moderate cosmetic requirements, and a production quantity that does not yet require a full long-life mold.
As an internal screening baseline, the part projection area is usually expected to be within 200 cm², and generally not more than 300 cm². Larger parts may exceed the practical range of standard mold bases, especially when clamp force, insert support, ejection balance, and runner layout become more demanding.
This makes the solution more suitable for:
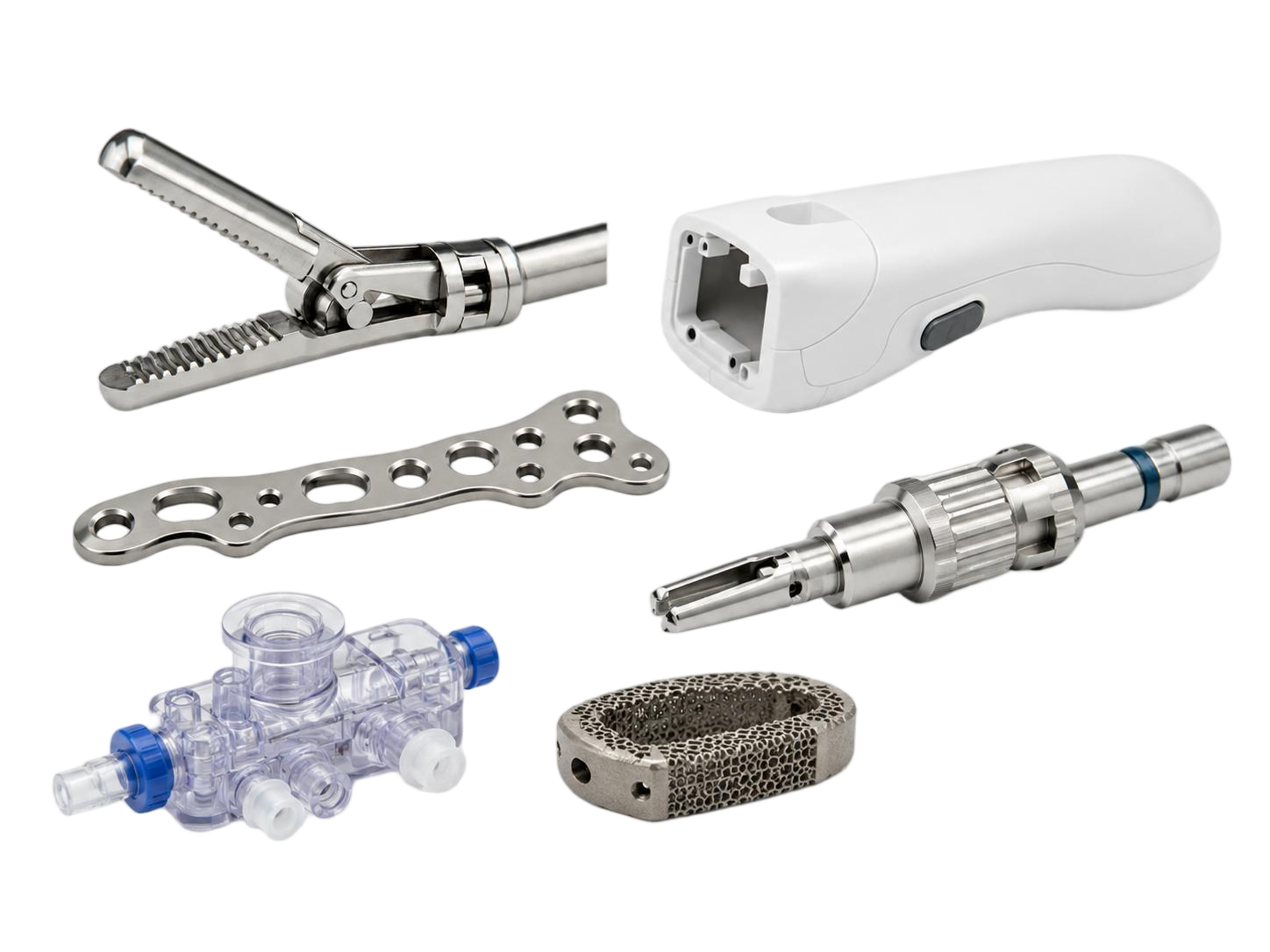
- Handheld medical device housings
- Small diagnostic instrument covers
- Internal structural brackets
- Battery covers or access covers
- Non-critical cosmetic enclosure parts
- Small transparent windows, when material and wall thickness are appropriate
It is less suitable for large desktop diagnostic equipment covers, large upper housings, or parts requiring extensive mold-base customization.
Structure: Keep Undercuts Controlled
The structure of the enclosure is often the main factor that decides whether shared mold base tooling is practical.
Medical device enclosures commonly include screw bosses, ribs, clips, battery compartments, display windows, ports, internal supports, sealing areas, and assembly features. These features are normal, but the mold structure must remain manageable.
A typical shared mold base project should avoid deep undercuts, multiple side actions, and complex moving mechanisms. A simple straight-pull design is preferred. One simple slider may be acceptable when the undercut is shallow and the mechanism can be integrated without losing the advantage of a standardized mold base. The uploaded technical note sets a practical reference: deep undercuts above 2 mm or more than two sliders/lifters usually make the solution unsuitable, while one simple slider with an undercut around 1.5 mm or less may still be feasible.
For enclosure design teams, this means early DFM work is important. A small change in clip direction, parting line, screw boss position, or port geometry may decide whether the project can use shared mold base tooling.
Cosmetic Requirements: Practical, Not Unlimited
Medical device enclosures often need a clean and professional appearance. This does not always mean a Class A surface. Many handheld or desktop medical products need controlled texture, consistent color, acceptable parting line placement, and reasonable management of weld lines and ejector marks.
Shared mold base tooling is more suitable for ordinary cosmetic surfaces, especially when the visible area does not require mirror-like gloss or strict Class A appearance. The technical note identifies ordinary cosmetic surfaces with Ra ≥ 1.6 μm as a more suitable range, while mirror-like Class A surfaces, such as high-end operation panels, should be avoided.
This does not mean appearance is ignored. It means appearance expectations must be realistic and discussed before tooling starts. The following points should be reviewed during DFM:
- Which surfaces are customer-facing?
- Where can the parting line be placed?
- Can ejector marks be hidden on internal surfaces?
- Will texture reduce visual sensitivity to flow marks?
- Is the material suitable for the expected surface finish?
- Are color matching and batch consistency required?
For medical enclosure projects, this early discussion prevents a common problem: choosing a low-cost tooling route while expecting full production-mold cosmetic performance.
Material Selection: Stable Materials Are Preferred
Material behavior directly affects mold feasibility. Shared mold base tooling is better suited to plastics with stable shrinkage, good flow, and predictable molding behavior.
For medical device enclosures, common engineering plastics such as PC/ABS, ABS, and PMMA may be appropriate depending on the application. PC/ABS is often used when the enclosure needs a balance of toughness and stiffness. ABS can be suitable for non-transparent structural covers. PMMA may be considered for transparent windows, but wall thickness and flow length need careful review.
High-viscosity or high-shrinkage materials are more difficult. Materials such as PPS, PEEK, or high-shrinkage PP can increase filling risk, dimensional variation, and mold compensation difficulty. These materials may still be used in medical or industrial applications, but they usually require a more dedicated tooling approach.
For each project, the material decision should be connected with:
- Mechanical strength
- Flame resistance
- Chemical resistance
- Sterilization or cleaning requirements
- Color and appearance
- Dimensional stability
- Assembly performance
- Regulatory or customer-specified material requirements
The tooling route should follow the material requirement, not the other way around.
Quantity: Best for Early-Stage and Low-Volume Needs
Shared mold base tooling is most valuable when the quantity is too high for CNC prototypes but not high enough to justify a dedicated mass-production mold.
A practical reference range is 50–5,000 parts. Below this level, CNC machining, 3D printing, or vacuum casting may be more cost-effective. Above this level, a full dedicated mold may offer better long-term economics, especially when the product design is stable and repeated production is expected.
This makes shared mold base tooling a strong option for bridge production. It gives the customer molded parts while the final production mold is being evaluated, modified, or prepared.
For medical device companies, this can support earlier product testing, investor demonstrations, distributor samples, pilot launches, or small-batch clinical-related builds.
Tooling Life: Short-Term Validation, Not Permanent Mass Production
The expected tooling life must be defined before the project starts. Shared mold base tooling should not be treated as a permanent replacement for a production mold.
The technical note identifies a typical mold insert life of up to around 30,000 shots for short-term validation needs. If the project requires more than 50,000 shots, higher-pressure molding, abrasive materials, or repeated long-term production, a dedicated mold with upgraded steel and structure should be considered.
This distinction is important. Shared mold base tooling is an engineering and business decision for a specific product stage. Once the design, market demand, and production volume are confirmed, a dedicated production mold may become the more appropriate solution.
When Shared Mold Base Tooling Should Be Avoided
A shared mold base solution should not be forced into unsuitable projects. It is usually not recommended when the enclosure has one or more of the following conditions:
- Large projection area above 300 cm²
- Multiple sliders or lifters
- Deep or multi-directional undercuts
- Strict Class A mirror-like cosmetic surfaces
- High-volume production above 5,000 parts
- High-viscosity or high-shrinkage materials
- Long-term production life requirements
These limits are not theoretical. They are linked to mold rigidity, clamping stability, insert support, ejection balance, material flow, dimensional compensation, and long-term tooling reliability.
Rapid MFG Online’s Engineering Approach
For Rapid MFG Online, shared mold base tooling is not presented as a universal shortcut. It is used as one option within a broader manufacturing decision process.
For medical device enclosure projects, we first review the 3D model, material requirement, visible surfaces, assembly structure, expected quantity, and project stage. The goal is to determine whether the enclosure is suitable for shared mold base tooling, whether the design needs DFM optimization, or whether a dedicated mold is safer.
A practical review usually includes:
- Part size and projected area
- Wall thickness and rib design
- Bosses, clips, windows, and openings
- Parting line and gate location
- Ejection risk
- Material shrinkage and flow
- Surface finish requirements
- Quantity and future production plan
If shared mold base tooling is suitable, the customer can reduce early tooling investment and obtain molded parts faster. If it is not suitable, identifying the issue early prevents tooling rework, cosmetic failure, assembly problems, and schedule loss.
Conclusion
Shared mold base tooling can be a practical solution for medical device enclosure projects, especially during prototype validation, bridge production, and early market launch. Its value is strongest when the part is within a controlled size range, the structure is not overly complex, cosmetic requirements are realistic, the material is stable, and the production quantity remains in a low-volume or pilot-production range.
The key is not to choose the lowest-cost mold. The key is to choose the tooling route that matches the project stage, technical risk, and production plan.
For medical device companies developing diagnostic equipment, handheld instruments, or low-volume enclosure products, shared mold base tooling can provide a faster and more economical path to real injection molded parts — when the engineering conditions are right.